
Kevin, a 37 year old truck driver, is shaking feverishly. He tries to tell his story, but between his gasping for air, the chattering of his teeth, and coughing spasms, he can barely speak.
As bad as he looks, his chest x-ray is worse. On the film Kevin’s lungs, which should be dark and air-filled, instead resemble a white snow storm, indicating severe pneumonia.

But this is not COVID. That illness would not explain Kevin’s rash. Covering his body and face are clear blisters atop an angry, red base.
I recognize this pattern, but I am not confident. I wonder if this is what the physicians of a generation ago meant by a “dew drop on a rose petal?”
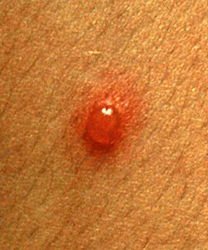
(The pathologists of old seemed to relish lovely descriptions of ugly things.)
With a little self-reproach, I remind myself that a pediatrician from a previous generation could have made this diagnosis instantly from fifty feet away. After all, those doctors saw chickenpox all the time.
On the other hand, I feel fortunate to have made the connection at all. Children younger than Kevin’s generation have never had chickenpox because of the introduction of a vaccine in 1995. As a result, the once ubiquitous disease is vanishingly rare, and I have little skill in diagnosing it. I suppose it is a great problem to have.
No Substitute
For most of human history, immunity to infectious diseases has been conferred solely by previous infections. Once a person had chickenpox, they were permanently “immune” to the infection, although it left some of its victims with disfiguring scars (not to mention the looming future possibility of shingles). By contrast in “naïve,” or unexposed, individuals and groups, new infectious diseases often ran rampant.
Kevin is one of the rare people his age who did not get chickenpox as a child, and so as an adult he has a particularly severe case. Fortunately there is an antiviral antibiotic that can be given in such a situation, and he will pull through.
But even in our age of such treatments, there is no substitute for the body’s own immune system. The greatest antibiotic – the best defense against a pathogen – is not made by a drug company. It is a white blood cell.
These miniscule warriors are the primary participants in tiny battles being fought inside our bodies on a daily basis – minute skirmishes that add up to life or death for you and me and even whole populations.
White cells and antibiotics kill microbes directly. In contrast, vaccinations do not directly impact germs. Instead they harness the immense power and precision of white blood cells and other components of our natural immune systems, helping our bodies to prepare beforehand for the onslaught of an infectious disease. Vaccines make us immune without ever having to suffer from an infection.
In a recent post I compared immunization to war games, like a simulated infection that trains your body to fight against the real infectious enemy when the time comes. The trick of vaccination is to provide enough stimulation to mobilize the immune system without harming the body.
The major differences in vaccines are how exactly they stage these war games. Several strategies are employed.
Live Vaccines
The earliest vaccine strategy, dating back perhaps 900 years, involves giving a live virus to a person, but in a controlled manner. In variolation real smallpox virus was used. However, this killer was introduced not through the normal airborne route, but through a small wound in the skin.
Instead of a potentially lethal, system-wide infection acquired from breathing in the virus naturally, the vaccine recipients suffered only a localized skin infection that gave them immunity to small pox.
What was the source of the virus used in variolation? There were no virology labs or biotech companies in the eighteenth century. Instead, individuals with smallpox sores were carried aboard ship to distant locations around the globe, like living vaccine factories, manufacturing the virus to stem outbreaks.
Before variolation (and the safer, easier smallpox vaccine developed by Dr. Edward Jenner in 1796) smallpox killed 3 in 10 people it infected and horribly disfigured many who survived.

It is estimated that this virus, now consigned to history by successful vaccination, killed 300 to 400 million people during the 20th century alone. Now you see why the smallpox vaccine is such a celebrated accomplishment! This is the most successful vaccine campaign in history and certainly one of the greatest public health triumphs of all time.
Strengths and Weaknesses
Today live vaccines consist of viruses or bacteria that have been weakened (attenuated) in some way. This strategy is akin to using captured and unarmed enemy combatants in a training exercise. Though they are shooting blanks, the hostiles still provide enough of a simulation to train the immune system effectively.
In theory this should afford a better semblance of a real infection for the body and induce a more robust immune response. Training against real troops can help defensive forces better study and recognize the patterns of hostile invaders.
The problem with live vaccines is that allowing an enemy, even a weakened enemy, into your territory runs some risks. Today there are more people than ever with impaired immune systems. Those who are receiving chemotherapy or drugs used to treat inflammatory diseases, like rheumatoid arthritis, lupus, or Crohn’s disease, and of course, or those with HIV infections, have downsized protective forces.
Against an ineffective military force, even unarmed foes in simulated combat can be dangerous. In training exercises, accidents happen, especially with poorly skilled participants.
Do you recall ingesting a sugar cube at the doctor’s office when you were a child? What was that strange treatment? It was the Sabin vaccine, a weakened form of a live polio vaccine. Since polio is contracted through oral ingestion, it stands to reason that mimicking not only the agent, but also the route, of the polio infection would generate the most effective immunity (by providing “mucosal IgA” protection right at the point of attack in the intestines).
A spoonful of sugar certainly helped the medicine go down!
This wonderful vaccine saved many children from the scourge of polio. However, the Sabin vaccine is currently out of use, because in very rare cases the live virus can get the upper hand over someone with reduced immune function. This can even cause a case of paralytic polio. Nowadays the original Salk polio vaccine, which uses a killed virus, is again preferred.
I administer live vaccines routinely today. Examples include the oral typhoid vaccine that I give to travelers before they set off to the developing world and the chickenpox vaccine given to children. These are great vaccinations. But we have to pick our battles carefully and avoid their use in the immunosuppressed population.
Protein Subunit Vaccines
Many successful vaccines take not an intact or weakened germ, but just a fragment, a protein from a germ, and introduce it into the body (by injection or ingestion). The intelligence officers of the immune system recognize this protein as foreign, and then design a system of smart weapons specially targeting it.
It is like taking a wing from a downed enemy aircraft with the insignia still on it and using it to drill military forces. Detection devices can be developed to register the enemy marking as soon as it enters your body’s airspace. That would be courtesy of the T cells, which memorize the protein signature, and immediately recognize it as unfriendly. Then antibodies, like smart weapons, latch onto the protein on the surface of a germ, destroying the attacker.
A New Hope
What about the new COVID-19 vaccines? How are they different? Some COVID-19 vaccines, like the Chinese and Russian ones, employ the traditional protein subunit platform.
But the new mRNA vaccine technology used in the Pfizer and the Moderna vaccines is different – and ingenious. This novel vaccine strategy devises an immune defensive strategy not by using a piece of the virus, but by using encoded information from the virus itself. It is as though we have stolen plans for the Death Star!

In my next post I will describe the defense system based on this novel vaccine technology and try and summarize what we know about its effectiveness and drawbacks.
Dr. Bill Maynard